Objective
To assess whether systematic complete revascularization with FFR-guided PCI following STEMI/very high risk NSTEMI leads to improved clinical outcomes compared to initial conservative management of non-culprit lesions.
Study
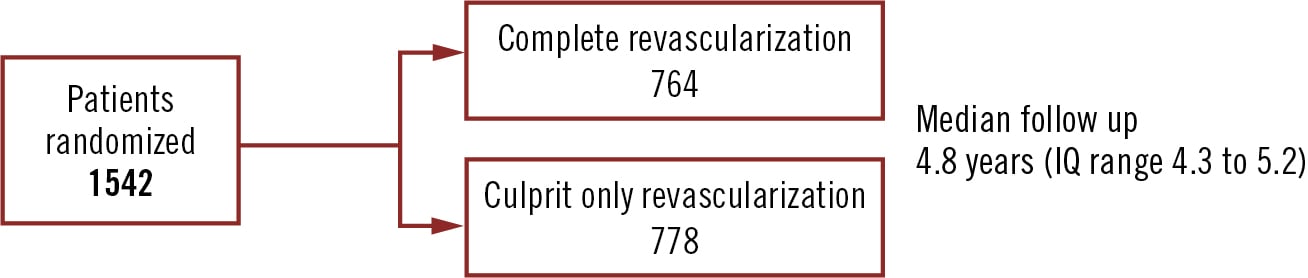
Randomised, open label, registry-based trial
Population
Patients presenting with STEMI or high risk NSTEMI undergoing urgent PCI and with multivessel coronary artery disease
Endpoints
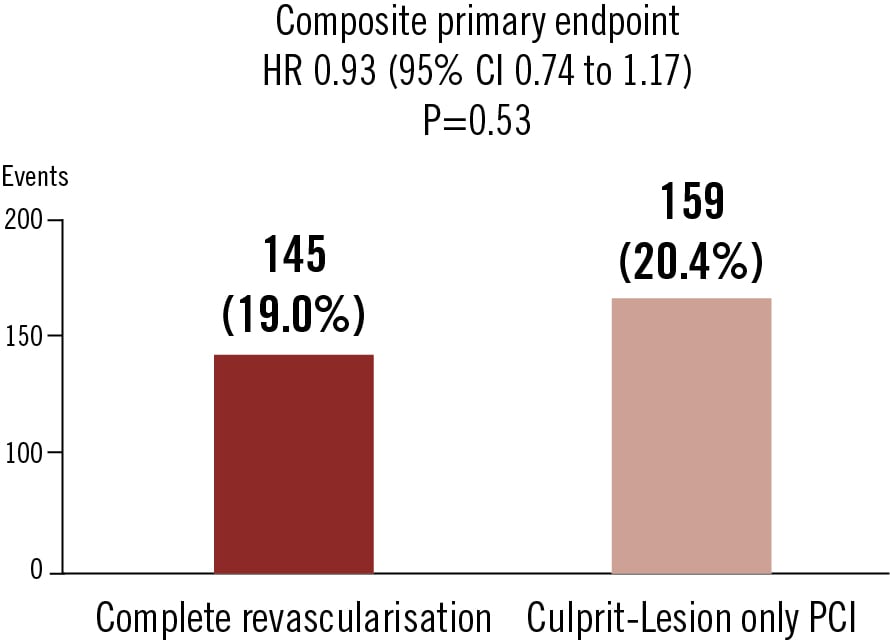
Combined endpoint of all-cause mortality, or myocardial infarction, or unplanned revascularization during a minimum follow-up of 2-3 years
Conclusion
FFR-guided complete revascularization of non-culprit lesions did not result in a lower risk of the primary endpoint than culprit-lesion only PCI in STEMI or very-high-risk NSTEMI at median 4.8 years follow up.
Böhm et al. N Engl J Med. 2024 April